-
Email info@jnans.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Neurosurgery Department, Viseu Dão-Lafões Local Health
Unit, Public Hospital, Portugal.
2Faculty of Medicine, University of Coimbra, Portugal.
*Corresponding author: Marcel Şincari
Neurosurgery Department, Viseu Dão-Lafões Local Health
Unit, Public Hospital, Portugal.
Email ID: sincari1973@gmail.com
Received: Feb 14, 2025
Accepted: Mar 21, 2025
Published Online: Mar 28, 2025
Journal: Journal of Neurology and Neurological Sciences
Copyright: © Cincari M (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Sincari M, Conceicao M, Sincari MD. Cystic meningiomas, literature review and case reports: Nauta classification modification. A pilot study. J Neurol Neuro Sci. 2025; 1(1): 1002.
Meningiomas of central nervous system are common lesion, but among them the cystic meningiomas are very rare tumors. We report two cases of cystic meningioma successfully treated and we propose the modification of the widely used Nauta classification of cystic meningiomas. The clinical results depend on meticulous preoperative diagnosis and surgical planning, enhancing the utility of modification of Nauta classification by adding bone invasion.
Keywords: Cystic; Meningioma; Dura; Brain.
Cystic meningioma is very rare with an incidence described is 9.6% [1]. According to other studies on cystic meningioma, the reported incidence is 1.6-11.7% [2-4]. It is more frequent on children, representing 12%-24% of pediatric meningiomas while it’s only of 2%-4% on adult, twice more on female probably due to hormonal factors [5].
Nauta in 1979 classified these tumors according to the location of the cyst relative to the tumor into 4 types. Type 1 cyst is contained wholly within the tumor and, being located centrally, or nearly so, is surrounded by macroscopic tumor throughout, type 2 he cyst is at the periphery of, but still wholly within the margins of the tumor, there being a microscopically visible attenuated rim of tumor cells along the peripheral margins of the cyst, type 3 the cyst again appears to be peripheral, and indeed actually lies within the adjacent brain rather than within the tumor itself, type 4 the cyst appears at the interface between the tumor and brain as a loculation of CSF in the subarachnoid space, and does not appear within either the tumor or brain itself [6]. There is no reference about adjacent bone invasion of the tumor.
There are several hypotheses for how cysts appear in meningiomas.
First hypothesis is degenerative phenomenon, the development of the cavity is due to intracellular regressive processes as vacuolar, myxomatous, mucoid and fatty degeneration [7,18]. Another hypothesis is ischemic: arteriolar hyalinization in the necrotic tissue of tumors that cause the intratumoral cavity [9]. The third hypothesis is previous intratumoral hemorrhage in angioblastic meningioma [8,10 13].
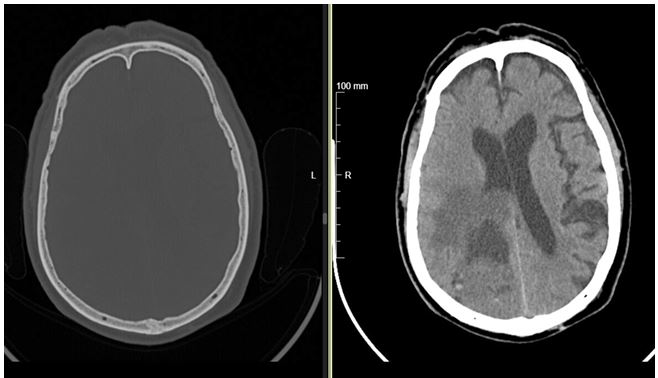
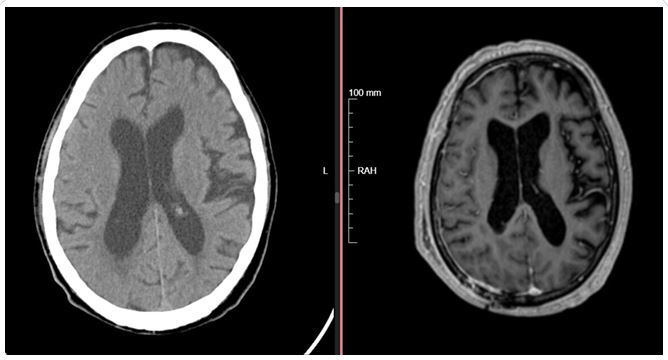
Case 1: A 76-year-old gentleman came to the emergency room for headaches and left hemiparesis, left homonymous hemianopsia, and mental confusion. An urgent CT scan re vealed a large lesion in the right occipital region, and an MRI of the brain showed an extraxial cystic right parieto-occipital neo plasm with extensive parenchymal edema. Due to an extraxial lesion in the right parieto-occipital region, the patient under went craniotomy and Simpson 2 excision.
Histologic examination revealed atypical meningioma, grade 2 (of 3) according to the WHO Classification. He followed radio therapy with total dose: 59.4 Gy 33 fractions/6.5 weeks. The patient remains under oncological and neurosurgical follow-up with a good recovery, postoperative MRI maintains dural thick ening adjacent to craniotomy.

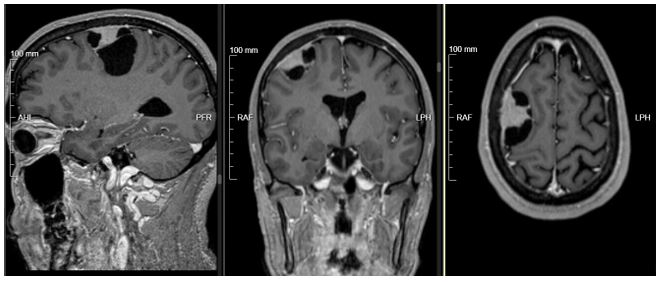
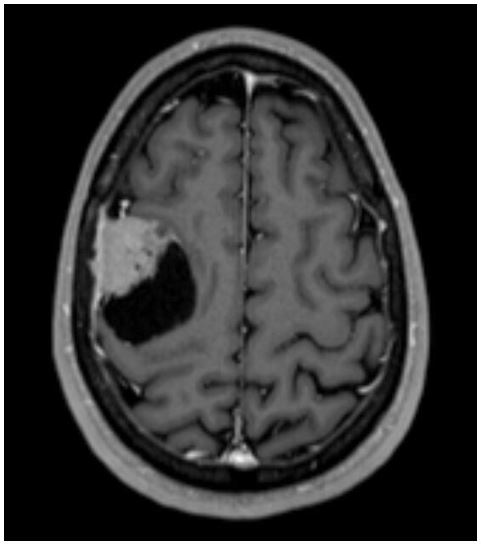

Case 2: A 45-year-old male presented with a clinical onset numbness the face, which progressed to a generalized tonic clonic seizure. He came to emergency services for these com plaints. A CT scan on admission revealed a large right parietal lesion, and an MRI of the brain indicated an extraxial neoplasm in the right occipital region with no edema. CT scan and MRI also detected bone invasion.
Given these findings, the patient underwent the following procedure: right parietal craniotomy guided by navigation, total microscopic resection of the posterior frontal tumor with dural involvement and bone invasion, removal of the dural flap and craniotomy, dural repartion using synthetic dura, and cranio plasty with a titanium plate. The procedure was uneventful. A postoperative CT scan showed complete resection of the lesion.
The preoperative diagnosis is a challenging task, MRI with contrast achieves a preoperative diagnostic accuracy of 80%, while CT scan approximately 50% [4,14,15]. The presence of an associated cyst is an uncommon imaging feature that may make it difficult to distinguish the tumor from a primary intra axial glial neoplasm and the presence of peritumoral edema can also be a misleading finding [16]. The presence of an intratu moral cyst can often create diagnostic challenges, resembling other neoplastic lesions [17-19]. The most frequent histologi cal subtype found was the meningothelial subtype [2,20,21]. Atypical meningiomas have the tendency to form a cyst, as opposed to other subtypes of meningioma [21,22]. MRI with diffusion-weighted imaging may be efficient in diagnosing the cystic meningioma [4,23], while the value of PET/CT in cystic meningioma requires further investigation and according to some studies it seems that diffusion-weighted imaging may be superior at distinguishing between the various types of menin gioma [4,24]. The presence of cystic components within and/ or around the mass usually suggests a diagnosis other than me ningioma. These tumors can be easily misdiagnosed as metas tases, gliomas and hemangioblastomas macroscopically in CT or MRI [25]. Although there are less dilemmas with MRI, cystic meningioma can easily be misdiagnosed, in about 20% of cases, particularly as glial tumor, metastasis, neuroblastoma or hae mangioblastoma [26].
Whether total cystic wall excision is necessary remains un clear. Author´s opinions are divided, some recommend that ex cision of the cyst wall is necessary [3,27], while other authors do not [11,29]. There are opinions that in the case of type II cystic meningiomas, every effort should be made to remove not only the mural nodule but also the cystic wall [2], other authors re ported a case of tumor recurrence in type II cystic meningioma in which the cystic wall was not completely removed [8,29-31], there are also reports that cyst wall components contain cells and complete removal of cystic components is essential [32].
We found in the literature only a sporadic description of cys t ic meningiomas with bony invasion, and curiously it was found in type II and III Nauta (with peripheral tumor adjacent to the bone [33-35], like it also was found in our second case. We pro pose to introduce a modification to Nauta classification, adding bone invasion, like type I, II, III, IV A-without bone invasion and B-with bone invasion.
Accurate diagnosis cystic meningioma is made through CT and MRI, but MRI remains the most effective on preoperative diagnostic, while the anatomopathological study is the only tool to confirm the diagnosis, allowing the correct management which should privilege a total resection as much as possible, total resection of the cyst and its prevents and diminish the risk of postoperative tumor recurrence.
The clinical results depend on meticulous preoperative diag nosis and surgical planning, enhancing the utility of modifica tion of Nauta classification by adding bone invasion.
Patient consent: Patient’s consent not required as patient’s identity is not disclosed or compromised.
Conflicts of interest: There are no conflicts of interest.
Use of Artificial Intelligence (AI)-assisted technology for manuscript preparation: The authors confirm that there was no use of Artificial Intelligence (AI)-assisted technology for as sisting in the writing or editing of the manuscript and no images were manipulated using AI.
