-
Email info@jnans.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Neurosurgery Department, Viseu Dão-Lafões Local Health
Unit, Public Hospital, Portugal.
2Faculty of Medicine, University of Coimbra, Portugal.
*Corresponding author: Marcel Şincari,
Neurosurgery Department, Viseu Dão-Lafões Local Health
Unit, Public Hospital, Portugal.
Email ID: sincari1973@gmail.com
Received: Feb 24, 2025
Accepted: Mar 24, 2025
Published Online: Mar 31, 2025
Journal: Journal of Neurology and Neurological Sciences
Copyright: © Sincari M (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Sincari M, Conceicao M, Sincari MD. Lumbar neurofibroma: Etiology, clinical presentation, surgical indications, and surgical technique. A focused view about surgical experience in Viseu-Portugal. J Neurol Neuro Sci. 2025; 1(1): 1003.
Lumbar neurofibroma is a benign neoplasm that originates from peripheral nerves, specifically from Schwann cells. While it can occur at various anatomical sites, its manifestation in the lumbar region has specific clinical and neurosurgical aspects, which are of great relevance for accurate diagnosis and effective treatment. This article addresses the causes, clinical presentation, indications for surgical treatment, and the surgical technique applied to lumbar neurofibromas, based on key studies and articles published in the last ten years.
Keywords: Neurofibroma; Lumbar; Root; Plexus.
Neurofibromas can be classified as either sporadic or heredi tary, with the latter often associated with Neurofibromatosis Type 1 (NF1), an autosomal dominant condition that results in multiple neurofibromas across various parts of the body. NF1 is caused by mutations in the NF1 gene located on chromosome 17, which codes for neurofibromin, a tumor suppressor protein. Patients with NF1 are predisposed to developing neurofibromas in various areas, including the spinal column, particularly in the lumbar region [1,2].
On the other hand, sporadic neurofibromas have no iden t ifiable genetic cause and can occur at any age, with higher prevalence in young adults [3]. Pathogenesis involves abnormal proliferation of Schwann cells, fibroblasts, and other peripheral nervous system cells.
The clinical presentation of lumbar neurofibromas can vary significantly depending on the size, location, and compression of adjacent structures, such as nerve roots and the spinal cord. Common symptoms include low back pain, radiculopathy, sen sory loss, or muscle weakness, with patients often affected by compression of spinal nerves exiting the lumbar spine [4].
In more severe cases, spinal cord compression can lead to more significant neurological symptoms, such as paralysis, uri nary and fecal dysfunction, and loss of reflexes. Pain is a pre dominant symptom, which may be continuous or intermittent, often exacerbated by movement of the spine [5].
Surgical indication
The main indication for surgery in cases of lumbar neurofi broma is the presence of progressive neurological symptoms or failure of conservative treatment. Surgery is indicated when there is evidence of nerve root or spinal cord compression caus ing debilitating pain, neurological deficit, or functional impair ment [1].
Furthermore, surgical removal is recommended in symp tomatic neurofibromas that interfere with the patient’s daily activities or when malignancy is suspected, a rare but possible condition that can occur in long-standing neurofibromas. The evaluation of malignancy is based on clinical and histological characteristics, with malignant transformation to neurofibro sarcoma being a severe complication that requires urgent in tervention [7].
Surgical technique
The surgical approach to lumbar neurofibromas must be carefully planned to minimize the risk of neurological injury and maximize tumor removal. The standard procedure involves lumbar laminectomy or extended laminectomy to ensure ac cess to the neurofibroma, which is often located in extradurally or paraspinal regions. The choice of laminectomy type depends on the tumor’s location and size [8].
The initial step in surgery involves careful exposure of the lumbar spinal structures and removal of the vertebral lamina, followed by identification and dissection of the neurofibroma. In cases of intradural neurofibromas, a more invasive approach may be necessary, with manipulation of the dura mater and nerve roots. The neurofibroma should be excised as completely as possible without compromising the integrity of the nerve roots, with attention to prevent damage to the spinal cord.
In some cases, Intraoperative Neurophysiological Monitoring (IONM) may be helpful to protect neurological structures during excision, especially in tumors located in difficult-to-access areas [2]. After tumor resection, the lumbar spine may be stabilized, if necessary, with instrumentation, depending on the extent of bone removal. The goal is to ensure functional recovery without additional neurological deficits.
In our series in two cases mini retroperitoneal approach was uses for tumor removal and in one case the tumor was ap proached through extended laminectomy.
Postoperative considerations
Postoperative management of patients undergoing lum bar neurofibroma resection includes pain control, neurologi cal monitoring, and early physiotherapy to promote mobility recovery. Full recovery may vary depending on the severity of preoperative symptoms and the extent of surgery. In NF1 cases, continuous monitoring is important to detect the development of new neurofibromas over time [4].
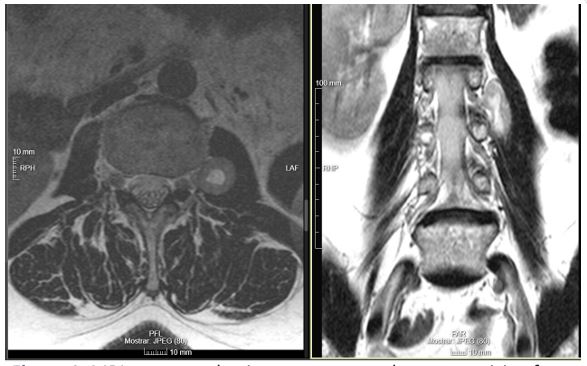
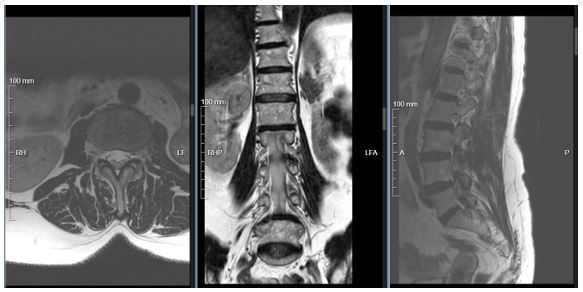
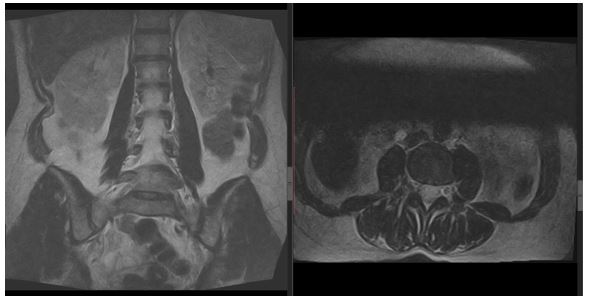
Case 1: 59 years old lady with history of renal TB treated, later left side nephrectomy due to lithiasis, presenting left side radicular pain L3 treated conservatively with no effect. Lumbar MRI showed extracanalar, intrapssoas muscle tumor, arising from left side L2 root (Figure 1). She was operated through left side mini retroiperitoneal approach with total removal of the tumor with resolution of complaints. Two years after surgery she is doing well, MRI revealed no tumor recurrence (Figure 2).
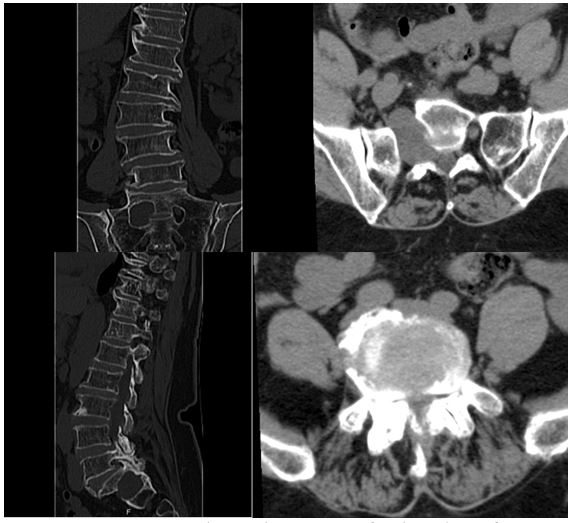
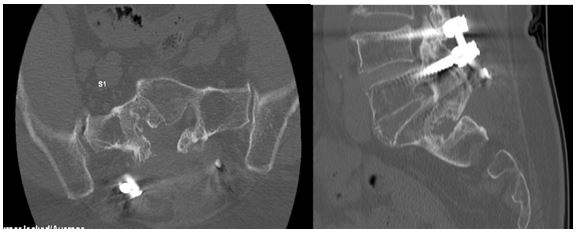
Case 2: 73 years old lady with a long lasting hystory of right side ciatic pain, worthened by association of progressive neu rologic claudication. CT scan showd severe L5-S1 stenosis and sacral errosion with enlagement of right side S1 foramina by a tumor arizing from extracanalar para of S1 root with evolution to presacral, retroperitoneal space (Figure 3). She was submit ted to psterior decompression of low lumar spine with fixation with transpedicular screws and S1 tumor total removal. 4 years after surgery she is doing well, complaining of numbness of righr leg, independent, using sporadically pain killers. CT scan 4 years after surgery shows no recurrence and the tumor bad is f illed with bone (Figure 4).
Case 3: 45 years old lady with complants of right side L2 pain with few effect with pain killers. MRI found left-side intrapssoas tumor adjacent to L3 root (Figure 5). She was operated through left-side mini retroperitoneal approach with total removal of tu mor and after two year MRI revealed no recurrence (Figure 6).

Lumbar neurofibromas represent a significant clinical and neurosurgical challenge, requiring early diagnosis and appropri ate management to prevent neurological complications. Surgi cal intervention is crucial in symptomatic cases, with tumor re section being the most effective strategy to alleviate symptoms and improve the quality of life of patients. Modern intraopera tive monitoring techniques and spinal stabilization options con tribute to a high surgical success rate.
Patient consent: Patient’s consent not required as patient’s identity is not disclosed or compromised.
Conflicts of interest: There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation: The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
