-
Email info@jnans.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Neurology, St. Joseph Medical Center,
Stockton CA, USA.
2Department of Neurology, University of Colorado Anschutz
School of Medicine, Aurora CO, USA.
*Corresponding author: Bertrand Liang
Department of Neurology, St. Joseph Medical Center,
Brookside Medical Building, Suite 2, 3132 March Lane,
Stockton, CA 95219, USA.
Tel: (209) 645-4005;
Email ID: bertrand.liang900@commonspirit.org
Received: Mar 05, 2025
Accepted: Apr 03, 2025
Published Online: Apr 10, 2025
Journal: Journal of Neurology and Neurological Sciences
Copyright: © Liang B (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Dalisay J, Rodriguez Y, Liang B. “Dancing fingers”: A case report of nitrous oxide poisoning with rare upper extremity presentation. J Neurol Neuro Sci. 2025; 1(1): 1004.
Nitrous oxide abuse is increasing globally particularly in the young, and manifests as neurologic symptoms typically affecting the lower extremities. We present a case of a patient with significant nitrous oxide abuse who presented with upper extremity symptoms of decreased sensation in the hand, with difficult to control spontaneous movement of the fingers bilaterally (“dancing fingers”). Laboratory examination revealed Jane Dalisay, DO1; Yamandu Rodriguez, MD1; Bertrand Liang, MD, PhD1,2* 1Department of Neurology, St. Joseph Medical Center, Stockton CA, USA. 2Department of Neurology, University of Colorado Anschutz School of Medicine, Aurora CO, USA. *Corresponding author: Bertrand Liang decreased vitamin B12 with elevated homocysteine and methylmalonic acid, with MRI revealing extensive demyelination of the cervical cord posteriorly and laterally. While nitrous oxide abuse often presents in the legs, suspicion should be high in young patients with anemia, sensory changes and evidence of upper motor neuron signs.
Keywords: Nitrous oxide; Substance abuse; Toxicity; Management; Upper extremity presentation; Subacute Combined degeneration of the cord.
Nitrous oxide is an anesthetic agent that has been used in a variety of medical and dental settings due to its rapid onset of action as well as high potency. However, it is also a drug of abuse, particularly in the younger population, and has been considered a “legal high” as it is available in the context of anes thetic practice and availability as propellant in whipped cream dispensers. Indeed, it has increased in use globally [1], and is one of the most frequently cited recreational drugs, often in combination with other illicit agents [2].
Nitrous oxide is not harmless. The drug is associated with significant neurologic issues, primarily due to depletion of vi tamin B12; it binds and oxidizes the vitamin and causes a func t ional deficiency [3,4]. The usual clinical scenario is associated with lower extremity symptoms, which range from an appar ent sensorimotor neuropathy to paresis and paresthesias with gait abnormalities [1,3]. We report a case of a patient with ni trous oxide abuse with primary upper extremity symptoms with chronic and acute increased usage.
A 23-year-old left handed man entered into the Emergency Department (ED) with complaints of tingling in his hands, and less so, in his feet. This had begun about a week prior to evalu ation, with vague muscle “twitches” in his arms. He particularly noted his hands weren’t “feeling right”, and as well could not feel the keys in his pocket when he reached for them with his left hand; he also noted over the past two days he could not feel his hand in his right pocket. He came to the ED because he noticed his fingers involuntarily “dancing” when he pulled them out of his pockets; only with effort could he stop the movement. The patient also noted he felt twitching of his thighs as he ar rived to the ED.
A CT brain scan was performed, which was read as negative for acute changes or stroke. Laboratory values included a nor mal metabolic panel, hemoglobin 13. 1g/L, hematocrit 39.9%, MCV 96.9 fl, negative COVID Ab, anti-T.pallidum, anti-HIV. Liver function tests were reported to be within normal range. Urine toxicology screen was negative. Initial exam by the ED staff re vealed, a heart rate of 89, respiratory rate of 16, temperature of 37°C; cardiac exam showed a regular rate and rhythm, clear lungs, no abdominal tenderness, and a non-focal neurologic exam except some mild weakness in the proximal lower extrem ities. Pulmonary function tests were reported to be normal. The impression by staff was a potential Guillain Barre Syndrome. Failed attempts at a lumbar puncture prompted Neurology to be consulted to obtain cerebrospinal fluid.
The patient was re-evaluated by Neurology. The patient noted he was a construction worker, and as well, a metal for mulation artist. He mentioned, “I need my hands – they’re my livelihood.” When asked explicitly about use of nitrous oxide, the patient admitted to chronic use of this “safe drug” over the past year “occasionally”, but had increased over the past three months to daily due to increased stress; his amount of use was unclear, since he had procured his own tank so was not using in dividual device administration (e.g. canisters), and instead used an inhalational mask.
On exam, the patient’s fingers spontaneously moved inde pendently with flexion/extension. He had saccadic EOM, with persistent lateral gaze nystagmus, with otherwise normal cra nial nerves. Slight proximal muscle weakness was present bilat erally in the lower extremities at 5-/5, with prominent bilateral pronator drift in the upper extremities, but no fasciculations were noted. The patient reported tingling in both hands. Pin prick exam was decreased in the upper extremities; there was anesthesia on the left to the mid-forearm and to the wrist on the right, with more tingling in the latter. Position sense was absent bilaterally in the hands, and perceived at the elbows, and slightly decreased at the toes requiring increased excur sions for detection. Reflexes were trace diffusely except at the ankles, where they were absent. Plantar responses were exten sor bilaterally. Finger-finger-nose testing showed missing of the target proximally and distally, with unsteady but more accurate heel-knee-shin testing. Fast finger movements were grossly ab normal bilaterally. Gait exam revealed a wide based station, but with intact on heel, on toe and casual gait with tandem gait fall ing to either side.
Additional laboratory studies showed a vitamin B12 level of 99 ng/L, with a folic acid level of 3.9 µg/L. Methylmalonic acid level was 170 µg/L, with homocysteine levels 52.1 µmol/L. Table 1 summarizes the laboratory data.
| Test | Value | Reference range |
|---|---|---|
| Hemoglobin (g/L) | 13.1 | 14-18 |
| Hematocrit (%) | 39.9 | 41-50.3% |
| MCV (fl) | 96.9 | 80-100 |
| COVID antibody | Negative | - |
| Rapid plasma reagin test (T. pallidum Antibody) | Negative | - |
| Urine toxicology screen | Negative | - |
| Vitamin B12 (ng/L) | 99 | 191-663 |
| Folic acid (µg/L) | 3.9 | 3.1-20.5 |
| Methylmalonic acid (µg/L) | 170 | <32 |
| Homocysteine (µmol/L) | 52.1 | <15 |
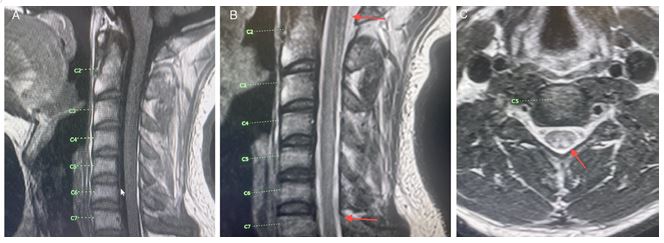
An MRI of the cervical spine was obtained. This revealed diffuse de myelination in the cervical spine, encompassing C1-C7 in the posterior and lateral segments. Figure 1 shows the results of the MRI.
The patient was diagnosed with vitamin B12 deficiency with symptoms associated with subacute combined degeneration of the spinal cord (“SCDC”). The patient was counseled that the use of nitrous oxide was the presumed source of his symptoms, and he underwent a week of parenteral vitamin B12 replace ment (1000 mg daily), followed by monthly injections. At fol low up six months later, the patient’s “dancing fingers” had im proved, as had the position sense and light touch in his hands.
Nitrous oxide (aka. “whippits”, “crackers”, “hippie crack”, “nang”, “balloons”) is typically a drug of abuse of the young. Case series have documented a median age of in the early 20’s, with a range of 12-30 years [1,5]. Overall, the use of nitrous oxide is increasing globally [3,6,7], often associated with other substance abuse [1]. The ease of access – whether through an esthetic means, or by canisters used for making whipped cream - and perception of being a “safe” drug has increased the pa t ients seen in the clinic and emergency departments [8].
Vitamin B12 deficiency is the result of nitrous oxide abuse, with oxidation of the cobalt ion in the vitamin with inactivation. Importantly, this can be noted with normal stores of vitamin B12, and hence it is important not to rely on the vitamin B12 levels alone, and evaluate the manifestations of the deficiency, viz. increased levels of homocysteine and methylmalonic acid [9]. Indeed, without vitamin B12, the homocysteine to methio nine conversion cannot be affected, which prevents in turn the methylation pathway of myelin proteins, as well as decreases in conversion of methylmalonic acid to metabolites to enter into the citric acid cycle for energy production [10]. Demyelination thus occurs in the spinal cord with predilection of the highly my elinated posterior columns and corticospinal tract, with charac teristic SCDC syndrome, with ischemia and decreased energy production suggested as causing neurotoxicity in the peripheral nervous system [10].
The clinical manifestation is typically associated with pares thesias and weakness of the lower extremities with gait abnor malities [11]. Oussaleh et al [12] noted almost all patients had at least one of these three neurologic symptoms, with others noting dominance of what is perceived to be central vs. periph eral nervous system symptoms [9]. While this may be a func t ion of the degree of usage, there are limited data on a specific dose response vis-a-vis symptomatology, although it has been hypothesized an existing lower vitamin B12 level is associated with more severe symptoms [1,3,8]. Similarly, some have deter mined hematologic findings, such as a macrocytic anemia can be present in a majority of patients [12] but others have found a less robust association [1]. As noted, vitamin B12 levels can be normal (up to 30% of cases) while high levels of homocysteine and methylmalonic acid are found in >90% patients [1,12]. Clini cal diagnosis relies on the laboratory findings combined with the MRI results, showing demyelinating disease particularly of the posterior and lateral aspects of the cervical spinal cord primarily (the “inverted v sign”) [12]. While a urine toxicology screen is often used to evaluate patients with suspected sub stance abuse, nitrous oxide does not appear in the urine and thus is not indicative of use with the exception of a potential indication of other substances, suggestive of a history of drug abuse [1,8].
Our case was unique in that the primary issue bringing the patient into the ED was his hand symptoms. Indeed, the patient specifically denied issues with gait or lower extremity weakness or paresthesias; it was his “dancing fingers” associated with the lack of sensation and tingling in the hands which prompted seeking care. Only with detailed neurologic evaluation were mi nor signs found in the lower extremities. However, what was suggestive in the patient was the initial hematologic findings combined with a history of profound loss of light touch and position sense, with the clinical manifestation of spontaneous movement of his fingers; signs of upper motor neuron involve ment of extensor plantar responses was supportive. It is unclear why the patient presented with predominantly upper extremity symptoms; this is rare in the context of nitrous oxide abuse, but has been noted in some case series [1,8,9]. In our case, the pa t ient had been using nitrous oxide chronically, but had acutely increased his usage over the past three months, with significant amounts given the availability of large doses because of hav ing his own tank/inhalational mask as a source. We posit this patient’s clinical presentation may have been because of the acute large doses that patient had used over the past several months, since it is usually smaller doses most patients utilize in container/canisters, rather than a mask. Further studies and experience will be required to assess whether this hypothesis can be verified. Regardless, with cessation of nitrous oxide use and vitamin B12 repletion, the patient did begin to improve in reports of his last follow-up six months later.
Vitamin B12 deficiency has been noted with other clinical scenarios. Abdominal surgery, copper deficiency/zinc excess, fo lic acid deficiency, as well as diet (being a vegetarian) have been associated with functional deficiency [13]. As well, other inflam matory and infectious disorders can affect or mimic SCDC such as autoimmune disorders, CNS demyelination disorders (e.g. multiple sclerosis), neurosarcoidosis, Guillain Barre Syndrome, HIV, neuro-syphilis as well as spinal cord vascular disease [8]. Many of these are associated with a transverse myelitis which can be associated with posterior column and corticospinal tract involvement. Most times careful historical information with the laboratory and physical exam can be helpful in discerning the etiology of a patient’s symptoms.
The treatment of nitrous oxide toxicity revolves around ces sation and replacement of vitamin B12. While the former is clear, the latter is less well defined [11]. Indeed, the variability noted of replacing the vitamin B12 is wide, and the question of whether to also replace folate if the levels are normal are unclear [8,11,13]. While it has been suggested vitamin B12 levels not be followed as the prime manifestation of therapy, and instead use homocysteine and methylmalonic acid, this also has not been carefully studied [14]. In our patient, we combined the advice of the poison control center with a review of the literature [11,15], to construct a treatment regimen for the patient for parenteral administration for a week with subsequent monthly injections. The duration of treatment has been debated from until symp toms remit to oral therapy lifetime [12,13,15] but again, this has not been well studied. The patient in our case opted for lifetime oral therapy with follow up with neurology.
We report a unique case of nitrous oxide poisoning with pre senting severe upper extremity symptoms in the hand as mani fest by “dancing fingers” with loss of position sense as well as light touch/pin prick sensation. While the lower extremities had mild signs noted on neurologic examination, the patient did not subjectively have any complaints associated with the legs. The lack of diagnostic testing via urine toxicology screen provided false reassurance of no substance abuse. The atypical symp toms neurologically perceived as weakness rather than sensory symptoms also created the perception of a primary neuropathic or neuromuscular syndrome, particularly given the diminished reflexes. Patients with nitrous oxide poisoning/abuse often have the classic lower extremity findings of gait abnormalities, weakness and paresthesias reminiscent of the SCDC syndrome; however, as this case illustrates, upper extremity findings with prominent examination findings localizing to the posterior and lateral spinal cord should prompt suspicion, especially in the context of a young person with a macrocytic anemia.
Acknowledgements: The authors thank Sid Gilman MD for helpful discussion, and the dedicated care team involved with the patient’s diagnosis and treatment.
Author contributions: JD, YR conceived, collected data and wrote/reviewed the manuscript; BL conceived, collected data, wrote/reviewed and supervised the creation of the manuscript.
Statements: Consent was obtained or waived by all partici pants of this study. All authors have declared no financial sup port was received from any organizations for the submitted work; that no conflicts of interest presently or within the pre vious three years exist with any organizations that might have an interest in the submitted work; and there are no other rela t ionships or activities that could appear to have influenced the submitted work.
