-
Email info@jnans.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Neurology and Psychiatry, Assiut University Hospital, Assiut, Egypt.
2Department of ENT, Audiology Unit, Assiut University Hospital, Assiut, Egypt.
*Corresponding author: Sherifa Ahmad Hamed
Department of Neurology and Psychiatry, Assiut University
Hospital, Assiut 71516, Egypt.
Email ID: hamedsherifa@aun.edu.eg & hamed_sherifa@yahoo.com
Tel: +2-088-2085106; Fax: +2-088-2333327
Received: Mar 31, 2025
Accepted: May 23, 2025
Published Online: May 30, 2025
Journal: Journal of Neurology and Neurological Sciences
Copyright: Hamed SA et al. © All rights are reserved
Citation: Hamed SA, Abd-El Hamed M, Oseily AM, Mohamed MKS. Assessment of auditory perceptual functions in patients with Parkinson’s disease. J Neurol Neuro Sci. 2025; 1(1): 1007.
Background: Hearing impairments are manifestations of Parkinson’s Disease (PD). We aimed to assess Central Auditory Processing (CAP) functions with PD and their predictors.
Methods: This was a cross-sectional study. It included 35 patients (male=21; female=14). The severity of PD was assessed using modified Hoehn and Yahr Scale. The severities of depression and cognitive manifestations were assessed using Beck Depression Inventory II (BDI-II) and Mini Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA). Participants underwent audiometry and testing of CAP using Dichotic Digit (DDT), Duration Pattern (DPT) and Speech In Noise (SPIN) tests.
Results: Patients had age of 56.66±11.05 yrs and duration of PD of 4.77±2.73 yrs. Compared to controls (n=25), patients had poor cognition [MMSE: 20.98±2.36, P=0.001; MoCA: 18.41±3.00, P=0.001], hearing impairment at high frequencies (4000 HZ), higher Speech Reception Threshold (SRT) (P=0.001) and worse performance in DDT, DPT and SPIN (P=0.0001). These impairments were independently correlated with cognitive deficits (DDT: P=0.036; DPT: P=0.050, SPIN: P=0.023).
Conclusions: CAP dysfunctions occur in early stages of PD. They include impairments in auditory discrimination, spatial perception, binaural integration, temporal ordering or sequencing, and selective attention. The DDT, DPT and SPIN are useful battery measures for testing CAP with PD. Dopamine deficiencies in PD at different auditory pathway levels including the brainstem and cortico-subcortical level and neurodegenerative diffuse PD pathology are the causes of CAP impairments.
Keywords: Parkinson’s disease; Hearing loss; Cognition; Auditory perception; Central auditory processing.
Parkinson’s Disease (PD) is a common neurological disorder with an estimated prevalence of 5.72 per 1000. PD is known by its triad of motor manifestations (rigidity, bradykinesia and rest tremors) and postural/balance disturbances [1]. PD also has Non-Motor Manifestations (NMMs) which occur early in the course of the disease or even years before the appearance of motor manifestations. The most common NMMs of PD include cognitive deficits [2,3], autonomic dysfunctions [4] and mood disorders [5]. Cognitive manifestations in PD range from Mild Cognitive Impairment (MCI) up to Dementia (PDD). MCI has been reported in ~40% in early stages of the disease [2]. Dementia has been reported in ~46% with disease duration exceeding 10 years and in up to 80% in late stages of the disease [3]. Attention and execution functions are affected in early stages of the disease while episodic memory is typically mild and presented late in the course of the disease [2]. The pathogenesis of cognitive dysfunction in PD involves loss of dopaminergic and non-dopaminergic neurons and dysfunction of multiple neurotransmitters (e.g. acetylcholine, norepinephrine and serotonin) and pathways. Studies reported that striatal dopamine reduction in PD causes decreased dopamine level in the prefrontal cortex [6,7]. Also, acetylcholine depletion is a cause of cognitive dysfunction in PD. Studies reported degenerations of the cholinergic neurons in PD, including the nucleus basalis of Meynert (Nbm), Medial Septal Nucleus (MSN), the Pedunculopontine (PPN) and Lateral Dorsal Tegmental (LDT) (or PPNLDT) neurons (which are brainstem projection neurons), and the Striatal Cholinergic Interneurons) (SChIs) (i.e. prefrontal cortex and frontostriatal circuit) [7,8].
Impairments of different perceptual functions (visual, auditory and olfactory and somatosensory) have also been reported with PD [9-11]. Impairments of peripheral and central auditory perceptions have been reported in PD. Evidence of peripheral hearing impairment with PD came from the complaints of hearing loss and the finding of abnormalities in objective hearing tests. Studies reported higher pure tone detection threshold in screening audiometry (PTA) [9-15] and lower amplitudes of Acoustic Emissions (OAE) [10] in patients with PD compared to age-matched healthy controls. Evidences for central hearing impairment with PD came from complaints of difficulty of hearing and understanding of speech particularly in noisy environments [9,10,16], disturbed perception of the characteristics of one’s own and other’s voices and speech and disturbed perception of emotional and syntactically relevant prosody [17,18] and the finding of significant abnormalities in the battery measures of central hearing processing. These abnormalities included increased Speech Reception Thresholds (SRT) in quite [11,19] and noise [20-22], impaired temporal spatial auditory processing as ordering or sequencing [23,24] and reduced spatial hearing sensitivity in divided and selective attentions [16,25-27]. The impairment of central auditory perception in presence of intact peripheral hearing can cause difficulty to locate sounds, hear speech clearly, extract a meaning from spoken sentences or messages and can interfere with listening in noisy conditions and poor social communication [19].
The pathogenesis of auditory perceptual dysfunctions in PD has been attributed to (a) Dopamine deficiency at different levels of the auditory system (cochlea, brainstem and the corticosubcortical levels). Dopamine is a neurotransmitter involved in sensory processing. It has a modulatory role in auditory processing [28]. (b) Degeneration of auditory neural structures and pathways at different neural levels by PD pathology (Lewy body, α-synuclein and Tau pathologies) [29]. (c) Degeneration of the cholinergic neurons by PD pathology and dysfunction of the prefrontal cortex and frontostriatal circuit, a high-order auditory processing (i.e. auditory cognitive perception) [30]. Alphasynuclein was found in the cholinergic medial olivocochlear system in patients with PD [31].
Few studies have been conducted on patients with PD for assessment of central auditory perception and their results were controversial. The contradictory results preclude the need for more clinical research work using the replicable and available measures to test auditory processing. Therefore, the work in this study was aimed to (a) assess central auditory perceptual function in a group of patients with PD using a battery of measures for evaluation of central auditory processing, and (b) determine the variables which were associated with central auditory perceptual dysfunction.
Study settings and participants
This was a cross-sectional study. It included 35 patients (male=21; female=14; age range=38–65 years) with idiopathic PD and 25 healthy individuals (male=17; female=8) matched for age (range=45–60 years), gender, educational level and socioeconomic status. Patients were recruited from the out-patient clinic of the department of Neurology and Psychiatry, Assiut University Hospital, Assiut, Egypt. Controls were recruited from the general population. Excluded from the study were individuals (1) ≥75 years old, (2) with manifest hearing loss, (3) with history of dementia or other central nervous system or systemic diseases, (4) with diagnosis of a psychiatric disorder, (5) with inner ear pathology or previous ear surgery, previous exposure to unsafe noise, or on regular use of known ototoxic drugs, and (5) with family history of hereditary hearing loss.
The protocol of the study was approved by the medical research ethics committees of the Faculty of Medicine, Assiut University, Assiut, Egypt. (ID#: AU-FM_Neuro_2020). Patients provided informed consents for participation.
Assessment
Evaluation for patients was done during the “On Phase of Medication”.
Sample collection
Participants underwent baseline medical, neuropsychiatric and audiological histories and examinations. The collected data included demographics (age, sex, educational level and socioeconomic status), duration of PD, severity of PD, therapeutic drugs and interventions and comorbid medical or surgical conditions. Low education level was defined as illiterate, could read or had primary or secondary school and higher education was defined as high school, collage, etc. Evaluation of socioeconomic state was done using the Socio-Economic Scale. Its total scoring is 30. The levels of socioeconomic status were classified as high (score = >25 to ≤30), middle (score = >20 to ≤25), low (score = ≥15 to <20), or very low (score = <15) [32].
Procedures
Assessment of the severity of PD: The severity of PD was assessed using the modified Hoehn and Yahr (H & Y) Scale [33]. They include Stag 1: Unilateral involvement; Stage 1.5: Unilateral and axial involvement; Stage 2: Bilateral involvement without postural instability; Stage 2.5: Mild bilateral disease with recovery on pull test; Stage 3: Mild/moderate bilateral disease and postural instability but physically independent; Stage 4: Severe disability but can walk or stand without assistance; and Stage 5: Wheelchair bound or bedridden.
Behavioral psychometric testing
Beck’s depression inventory – II (BDI-II): The severity of depressive symptoms was assessed using BDI-II. It is a 21-item questionnaire. According to the scores of BDI-II, the severity of symptoms was classified as no/minimal symptoms (score: 0 to 13), mild (score: 14 to 19), moderate (score: 20 to 28) or severe (score: 29 to 63) [34].
Cognitive testing: Cognitive function was assessed using the Arabic translated and validated versions of Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) test. Each took ~10-15 min to be administered.
The questions of MMSE were grouped into 7 categories to assess different domains of cognition which included attention, concentration, orientation to time and place, short-term, long-term and verbal memory, calculation and visuospatial skills. The maximum score of MMSE is 30. As most participants had low education, we deducted the two points which test reading and writing and the MMSE score was calculated as 28 (instead of 30). Cognitive deficits were considered with scores less than 22 (instead of 24). The severity of cognitive deficits was classified into normal (score: 22 to 28), mild (MCI) (score: 19 to 21), moderate (score: 8 to 18) and severe (score: 8) [35]. The tasks in MoCA included assessment of visuospatial/executive function, naming, delayed memory, attention, language, abstraction and orientation. Its total score is 30. We deducted the 5 points which test visuospacial and visuoconstructive abilities and the MoCA score was calculated as 25 (instead of 30). The severity of cognitive deficits were classified into normal (score: 20 to 25), mild (score: 12 to 19), moderate (score: 4 to 11) and severe (score: <4) [36].
Auditory testing
Basic audiologic evaluation: This included otoscopic ear examination, screening audiogram (pure tone audiometry or PTA), acoustic reflex (Interacoustics model AC40, v.1.28, Assens Denmark), tympanometry (200 top –400 dapa) and speech audiometry. PTA (air conduction) was assessed for each ear at frequencies of 250, 500, 1000, 2000 and 4000 Hz. The severity of hearing loss (over the whole frequency range) was categorized into normal (–10 to 15 dB HL) and slight (16 to 25 dB HL), mild (26 to 40 dB HL), moderate (41 to 55 dB HL), moderately severe (56 to 70 dB HL), severe (71 to 90 dB HL) and profound (≥ 91 dB HL) deficits [37]. Speech audiometry included Speech Discrimination Scale (SDS) and Speech Reception Threshold (SRT) tests. In SDS test, the subject was asked to understand and repeat a set of 25 monosyllables. Normal SDS was considered if SDS score was 100%. In SRT test, the subject was asked to repeat a list of spondaic disyllable words, followed by subsequent reduction in the sound intensity level. This was done to determine the lowest volume which the subject can hear and recognize speech. SRT was considered normal if SRT was ≤25 dB HL [37].
Central auditory processing testing: This was done using the Arabic validated and reliable computerized versions of the free recall Dichotic Digits (DDT), Duration Pattern (DPT), and Speech Perception in Noise (SPIN) tests (https://auditecincorporated. files.wordpress.com/2015/03/quality.jpg; Auditec, Inc.). In each test, the audio track from CDs was triggered by a program written and played through a digital-to-analog converter with an amplifier connected to the inputs of a clinical audiometer. The sounds were then delivered to the listener via insert earphones. In this work, for each patient, tests were conducted at 40 dB above the threshold level at which speech was detectable. Responses were indicated by the participant using a verbal response. Participant responses were entered by the examining audiologist using an appropriate printed score sheet. A participant was encouraged to take breaks, and testing was discontinued if fatigue or frustration was evident. The DDT, DPT, and SPIN tests were done over the course of three separate sessions.
In DDT, we used the two-digit test. Each list of the test contained 20-digit pairs. The subject was asked to repeat all digits that were heard in both ears, without specifying in which ear the digit was heard or the order of digits’ presentation. The results were presented as the percentage of the correctly repeated digits from all presented digits. The normal score ranged from 85% to 100% [38,39]. DDT was chosen to assess auditory spatial perception, binaural integration and divided attention.
In DPT, presentation was done with 1 kHz tones in sequences of three, where each tone had duration of either 250 millisecond (short) or 500 milliseconds (long) with 300 milliseconds intervals between the tones in the sequence of the three tones. DPT test was done using bilateral presentation. The subject was asked to label each of the tone durations as either short (S) or long (L) in each series, for example, “short, long, long.” There were six possible combinations of the three tones (SSL, LLS, LSL, SLS, LSS and SLL). The Duration Pattern Test (DPT) consists of 40 random sequences of three tones. To be scored as correct, each three-item sequence of the tones had to be identified with the lengths in the correct order [38,39]. The normal score ranged from 68% to 80%. DPT was chosen to assess tasks of temporal ordering or sequencing which refers to the processing of multiple auditory stimuli in their order of occurrence.
In SPIN test, presentation was done to each ear using 2 lists of 25 pre-recorded sentences in the presence of background masking speech noise (multi-talker babble). These sentences were reflective of real-world listening conditions and the use of context. The test is adaptive in that the loudness of the speech fluctuates during the test while the multi-talker babble level remains constant. The number of correctly identified sentences was calculated as a percent correct score as average from both ears [40,41]. The normal score ranged from 90% to 100%. SPIN test was chosen to assess selective auditory attention. It also provided assessment of some aspects of temporal processing (e.g. the degradation of temporal aspects, as decoding of speech signals, ordering and resolution) and memory.
Statistical analysis
Data were analyzed with SPSS (IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp). Data were expressed as mean (SD). Comparative statistics were performed using independent sample t-test. Post hoc Bonferroni was applied to correct for multiple variables. Correlation analyses between variables were conducted using Spearman’s correlation coefficient. Regression analyses were done to determine the variables which were significantly and independently associated with central auditory processing results. Univariate Analysis of Variance was done (age was fixed) to determine the associations between scores of DDT, DPT and SPIN tests (i.e. the dependent variables) and demographics and clinical variables and scores of BDI-II and MoCA (i.e. independent variables). Variables with significance in univariate analysis were included in the multivariate model. Significance was considered if P>0.05.
Demographics and clinical characteristics
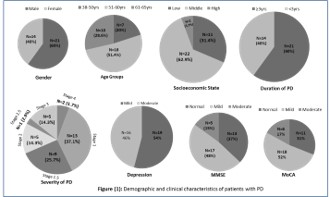
This study included 35 patients with PD (male/female = 1.5/1) and 25 healthy subjects. Patients had mean age at presentation of 56.66±11.05 years (versus 50.32±8.35 for controls, P=0.460). They had mean duration of PD of 4.77±2.73 years (range=1–10 years). The majority (60%) have duration of PD of ≤3 years. The majority were married (91.4%, n=32), of low education level (80%, n=28) and of low/middle socioeconomic states (94.29%, n=33). Family history of PD was found in 27 patients (77%). The mean score of Hoehn and Yahr (H & Y) Score was 2.14±0.89. Twenty-four patients (68.57%) had less severe stages of the disease (stages: 1, 1.5 and 2) (Figure 1). Patients (n=35) were on regular treatment for at least 6 months before inclusion with levodopa/carbidopa (Sinemet) with a mean dose of 604.64±57.21 mg/d (range=275–825 mg/dl) divided into 2 to 4 times per day.
Results of psychometric testing
None of the patients had major depression. Sixteen patients (46%) had moderate symptoms of depression and 19 (52%) had mild symptoms. None of the patients had dementia or significant cognitive symptoms. Mild Cognitive Impairment (MCI) was reported in 48% (n=17) (by MMSE) and 52% (n=12) (by MoCA) and moderate cognitive impairment was reported in 15% (n=5) (by MMSE) and 17% (n=6) (by MoCA). Normal scores were reported in 37% (n=13) (by MMSE) and 31% (n=11) (by MoCA). Cognitive testing showed that patients had significant lower global cognitive scores compared to controls (P = 0.001) [Patients: 20.98 ± 2.36, range: 8-26 by MMSE and 18.41±3.00, range: 4-22 by MoCA versus controls: 25.07±2.00, range: 22-28 by MMSE and 20.97±3.24, range: 16-25 by MoCA]. There was concordance between the results of MMSE and MoCA tests. Also, there was a significant positive correlation between MMSE and MoCA scores (P=0.0001) (Figure 1).
Results of audiology testing
The results of PTA recorded from each ear at different frequencies, speech audiometry, tympanometry and acoustic reflex were shown in Table 1. It showed that patients had significant shift in hearing thresholds at high frequencies (4000 HZ) compared to healthy controls. All had type A tympanometry and 60% (n=21) had bilateral absent acoustic reflex. No significant differences in were found in SDS scores in patients compared to controls. Patients had significantly higher SRT compared to controls (P=0.001).
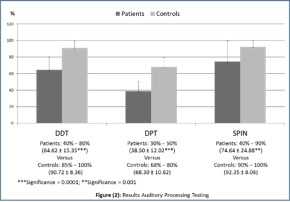
Compared to controls, patients had significantly lower scores in DDT, DPT, and SPIN tests (P=0.0001 for all) (Figure 2). Each patient had abnormalities in at least two of the battery tests. Twelve patients (34.29%) had DDT scores ranged from 40% to 55% and 23 (65.71%) had DDT scores ranged from 60% to 80%. Thirty patients (85.71%) had DPT scores ranged from 30% to 45% and 5 patients (14.29%) had DPT scores ranged from 50% to 55%. Twenty-one patient (60%) had SPIN scores ranged from 40% to 55% and fourteen (40%) had scores ranged from 60% to 90%. No significant differences in demographics, clinical and audiologic (peripheral and central) characteristics in relation to gender or age groups.
Comparative statistics between patients without and with cognitive deficits
No significant differences were identified between patients without (n=13) and with (n=22) cognitive deficits in demographics, clinical characteristics, PTA, SDS score, SRT and scores of DDT, DPT and SPIN tests.
They were as follow: (a) increasing age was significantly correlated with high scores of H & Y, BDI-II scores, and SRT levels and low MMSE and MoCA scores, (b) high scores of H & Y were significantly correlated with increasing age, high BDI-II scores and low MMSE and MoCA scores, (c) low MMSE and MoCA scores were significantly correlated with increasing age, high scores of H & Y and BDI-II. (d)Significant correlation was identified between scores of MMSE and MoCA, (e) high SRT values were significantly correlated with increasing age and low SDS scores (Table 2). (f) Significant correlations were identified between low scores of DDT, DPT and SPIN tests and increasing age, high H & Y scores, high BDI-II scores, high SRT values and low MMSE and MoCA scores. (g) Significant correlations were identified between scores of DDT, DPT and SPIN tests (Table 3).
Univariate analysis between scores of DDT, DPT and SPIN tests and demographics, clinical variables, SDS scores, SRT values, BDI-II scores, MoCA scores showed that only scores of MoCA test (DDT: P=0.036; DPT: P=0.050, SPIN: P=0.023) and higher SRT values (DDT: P=0.048; DPT: P=0.050, SPIN: P=0.043) were significantly and independently associated with lower scores in DDT, DPT and SPIN tests (Table 4).
| Variables | Patients (n=35) | Controls (n=25) | P-Value | |
|---|---|---|---|---|
| PTA | ||||
| AC: Reception Threshold (dB HL) | AC: Reception Threshold (dB HL) | |||
| Right Ear | Left Ear | |||
| 250 HZ | 20.00-55.00 (27.65±8.81) | 20.00-50.00 (28.57±8.45) | 15.00-30.00 (23.45±6.02) | |
| Normal | 15 (42.86%) | 12 (34.29%) | - | P1: 0.350 |
| Slight | 12 (34.29%) | 16 (45.71%) | - | P2: 0.382 |
| Mild | 8 (22.86%) | 7 (20%) | - | |
| 500 HZ | 20.00-55.00 (30.15±10.55) | 20.00-50.00 (31.14±9.40) | 20.00-40.00 (28.30±6.35) | |
| Normal | 12 (34.29%) | 10 (28.57%) | - | P1: 0.288 |
| Slight | 15 (42.86%) | 18 (51.43%) | - | P2: 0.326 |
| Mild | 8 (22.86%) | 7 (20%) | - | |
| 1000 HZ | 10.00-65.00 (32.50±10.75) | 15.00-60.00 (32.86±10.45) | 10.00-40.00 (30.68±8.24) | |
| Normal | 18 (51.43%) | 16 (45.71%) | P1: 0.350 | |
| Slight | 11 (31.43%) | 10 (28.57%) | P2: 0.320 | |
| Mild | 9 (25.71%) | 9 (25.71%) | ||
| 2000 HZ | 20.00-70.00 (42.35±16.11) | 20.00-70.00 (40.86±14.88) | 20.00-55.00 (38.80±10.56) | |
| Normal | 6 (17.14%) | 8 (22.86%) | P1:0.328 | |
| Slight | 13 (37.14%) | 13 (37.14%) | P2: 0.268 | |
| Mild | 16 (42.11%) | 14 (40%) | ||
| 4000 HZ | 20.00-100.00 (45.56±21.86) | 25.00-100.00 (50.29±19.37) | 20.00-50.00 (40.60±12.45) | |
| Normal | 0 | 0 | - | |
| Slight | 0 | 0 | P1: 0.032 | |
| Mild | 28 (80%) | 32 (91.43%) | - | P2: 0.018 |
| Moderate | 7 (20%) | 3 (8.57%) | - | |
| Variables | Speech audiometry, tympanometry and acoustic reflex | P-Value | ||
| Right Ear | Left Ear | |||
| SDS | 56.00-100.00 (86.66±13.02) | 56.00-100.00 (92.056±12.94) | 92.00-100.00 (95.25±5.20) | |
| Normal (100%) | 5 (14.3%) | 5 (14.3%) | - | |
| Mild (85-95%) | 12 (34.29%) | 13 (37.1%) | - | P1: 0.328 |
| Moderate (70-80%) | 12 (34.29%) | 11 (31.4%) | - | P2: 0.258 |
| Poor (60-70%) | 6 (17.1%) | 6 (17.1%) | - | |
| SRT | 10.00-60.00 (52.00±8.03) | 10.00-60.00 (55±6.67) | 10.00-45.00 (20.00±3.43) | |
| Normal (21-40 dB) | 6 (17.1%) | 3 (8.6%) | - | P1: 0.001 |
| Moderate (41-70%) | 29 (82.9%) | 32 (91.4%) | P2: 0.001 | |
| Tympanometry | Type A (100%) | Type A (100%) | Type A (100%) | - |
| Acoustic Reflex | ||||
| Normal | 14 (40%) | 14 (40%) | 25 (100%) | |
| Absent | 21 (60%) | 21 (60%) | - | - |
SDS: Speech Discrimination Scale; SRT: Speech Reception Threshold Significance; P1: right ear of patients versus controls; P2: Left ear of patients versus controls.
| Age | Duration of Illness | H and Y | BDI-II | Right SDS | Left SDS | Right SRT | Right SRT | MMSE | |
|---|---|---|---|---|---|---|---|---|---|
| Age Correlation Coefficient Sig. (2-tailed) |
- - |
||||||||
| Duration of Illness Correlation Coefficient Sig. (2-tailed) |
-0.178 0.307 |
- - |
|||||||
| Modified H and Y Correlation Coefficient Sig. (2-tailed) |
0.570 0.0001 |
0.265 0.124 |
- - |
||||||
| BDI-II Correlation Coefficient Sig. (2-tailed) |
0.669 0.0001 |
0.117 0.504 |
0.668 0.0001 |
- - |
|||||
| Right SDS Correlation Coefficient Sig. (2-tailed) Left SDS Correlation Coefficient Sig. (2-tailed) |
0.136 0.437 -0.157 0.369 |
0.442 0.008 0.437 0.009 |
0.133 0.445 0.135 0.439 |
0.025 0.885 -0.062 0.724 |
- - 0.954 0.0001 |
- - |
|||
| Right SRT Correlation Coefficient Sig. (2-tailed) Left SRT Correlation Coefficient Sig. (2-tailed) |
0.422 0.012 0.331 0.052 |
-0.090 0.607 -0.098 0.576 |
0.180 0.300 0.082 0.640 |
0.430 0.010 0.325 0.057 |
-0.555 0.001 -0.559 0.0001 |
-0.609 0.0001 -0.568 0.0001 |
- - 0.903 0.0001 |
- - |
|
| MMSE Correlation Coefficient Sig. (2-tailed) |
-0.634 0.0001 |
0.145 0.406 |
-0.412 0.014 |
-0.540 0.001 |
-0.025 0.888 |
0.037 0.835 |
-0.168 0.334 |
-0.141 0.421 |
- - |
| MoCA Correlation Coefficient Sig. (2-tailed) |
-0.754 0.0001 |
0.095 0.586 |
-0.571 0.0001 |
-0.633 0.0001 |
0.041 0.815 |
0.052 0.768 |
-0.290 0.091 |
-0.309 0.070 |
0.685 0.0001 |
Modified H and Y staging scoring; Modified Hoehn and Yahr staging score; BDI-II: Beck's Depression Inventory – II; SDS: Speech Discrimination Scale; SRT: Speech Reception Threshold; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment.
| Testing | DDT Correlation Coefficient (Sig. 2-tailed) | DPT Correlation Coefficient (Sig. 2-tailed) | SPIN (Correlation Coefficient (Sig. 2-tailed) |
|---|---|---|---|
| DDT | - | 0.968 (0.0001) | 0.947 (0.0001) |
| DPT | 0.968 (0.0001) | - | 0.930 (0.0001) |
| SPIN | 0.947 (0.0001) | 0.930 (0.0001) | - |
| Age | -0.583 (0.0001) | -0.587 (0.0001) | -0.540 (0.001) |
| Duration of illness | 0.247 (0.153) | 0.259 (0.134) | 0.178 (0.305) |
| Modified H and Y scoring | -0.375 (0.027) | -0.427 (0.011) | -0.417 (0.013) |
| BDI-II | -0.557 (0.001) | -0.546 (0.001) | -0.504 (0.002) |
| SDS Right side Left side |
0.012 (0.946) 0.100 (0.567) |
0.020 (0.910) 0.089 (0.611) |
0.093 (0.594) 0.174 (0.318) |
| SRT Right side Left side |
-0.386 (0.022) -0.291 (0.090) |
-0.321 (0.060) -0.252 (0.145) |
-0.470 (0.004) -0.394 (0.019) |
| MMSE | 0.587 (0.0001) | 0.630 (0.0001) | 0.558 (0.0001) |
| MoCA | 0.616 (0.0001) | 0.643 (0.0001) | 0.635 (0.0001) |
| DDT | - | 0.968 (0.0001) | 0.947 (0.0001) |
Data are presented as correlation coefficient (significance [2-tailed]). DDT: Dichotic Digit Test; DPT: Duration Pattern Test; SPIN: Speech Intelligibility in noise; BDI-II: Beck's Depression Inventory – II; SDS: Speech Discrimination Scale; SRT: Speech Reception Threshold; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment.
| Sum of Squares | Mean Square | F | Significance | |
|---|---|---|---|---|
| DDT | ||||
| Corrected Model | 7216.835a | 248.856 | 2.940 | 0.116 |
| Intercept | .034 | .034 | .000 | 0.985 |
| Duration of illness | 11.872 | 11.872 | .140 | 0.723 |
| H and Y scoring | 98.585 | 98.585 | 1.165 | 0.330 |
| BDI-II | 3.237 | 3.237 | .038 | 0.853 |
| MoCA | 458.196 | 458.196 | 6.414 | 0.036 |
| SDS | 22.980 | 22.980 | .272 | 0.625 |
| SRT | 574.192 | 574.192 | 6.784 | 0.048 |
| DPT | ||||
| Corrected Model | 6592.237a | 227.319 | 3.020 | .110 |
| Intercept | .022 | .022 | .000 | 0.987 |
| Duration of illness | .357 | .357 | .005 | 0.948 |
| H and Y scoring | 39.874 | 39.874 | .530 | 0.499 |
| BDI-II | 10.711 | 10.711 | .142 | 0.721 |
| MoCA | 467.394 | 467.394 | 6.258 | 0.050 |
| SDS | 43.278 | 43.278 | .575 | 0.482 |
| SRT | 487.719 | 487.719 | 6.486 | 0.050 |
| SPIN | ||||
| Corrected Model | 6126.738a | 211.267 | 2.360 | .172 |
| Intercept | .956 | .956 | .011 | 0.922 |
| Duration of illness | .011 | .011 | .000 | 0.992 |
| H and Y scoring | 31.549 | 31.549 | .352 | 0.579 |
| BDI-II | 3.107 | 3.107 | .035 | 0.860 |
| MoCA | 412.651 | 412.651 | 7.610 | 0.023 |
| SDS | 14.279 | 14.279 | .160 | 0.706 |
| SRT | 419.181 | 419.181 | 6.683 | 0.043 |
| R Squared = .945 (Adjusted R Squared = .623) Age is a fixed factor | ||||
DDT: Dichotic Digit Test; DPT: Duration Pattern Test; SPIN: Speech Intelligibility in noise; Modified H and Y staging scoring; Modified Hoehn and Yahr staging score; BDI-II: Beck's Depression Inventory – II; SDS: Speech Discrimination Scale; SRT: Speech Reception Threshold; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment.
This work was conducted to evaluate central auditory perception in group of patients with PD. Previous studies which assessed central auditory function in patients with PD were few and their results were contradictory. In this study, we examined a homogenous group with PD. They were assessed during the “on phase of medication”. The majority was in their 4th and 5th decades of life, in early stages of PD and may had short duration of the disease. The results of psychometric and auditory tests of patients with PD were compared with age-matched healthy subjects. In this study, we evaluated peripheral hearing and cognition before testing central auditory processing to specifically exclude patients with significant hearing loss or cognitive deficits which could influence the results of central auditory processing. Examination of peripheral hearing was done using screening PTA. It showed that the majority of patients had mild hearing impairment at 4000 HZ compared to healthy controls. There were no differences in PTA results in relation to age, gender or severity of PD. Previous studies reported subclinical hearing loss in patients with PD at high frequencies (4000-8000 HZ). Some studies reported high rates of peripheral hearing loss in early-onset PD [10,12], while others reported high prevalence of increased pure-tone hearing thresholds in elderly patients with PD [9,11,13,15]. It has been suggested that these abnormalities indicate dysfunction of the basal cochlea. The increased hearing loss in elderly with PD has been suggested to be due to the combined effects of an age-related Sensorineural Hearing Loss (SNHL) or presbycusis and the neuropathological changes of PD. Presbycusis includes loss of basal cochlear hair cells [9,11,13,15]. It has been shown that dopaminergic neurotransmission involves many levels for auditory processing in response to auditory stimuli, including the cochlea, auditory brainstem, midbrain, thalamus, and cortex [42]. The Lateral Olivocochlear (LOC) efferents release dopamine in response to different stimuli which protect the cochlea from the glutamate excitotoxic damaging effect caused by auditory overstimulation. These efferents synapse on the Inner Hair Cells (IHCs) of the cochlea [42,43]. Studies which assess peripheral hearing using Otoacoustic Emission (OAE) analysis reported reduced OAEs amplitudes of in patients with PD compared to healthy controls [10,24]. The OAE analysis reflects the function of OHCs of the cochlea. The increased of OAEs amplitude after dopaminergic medications support incrimination of dopamine in dysfunction of the cochlear OHCs. The Medial Olivocochlear (MOC) efferents do not release dopamine.
The MOC efferents synapse on the OHCs of the cochlea. It has been suggested that the synapses between the LOC and MOC may explain the modulatory effect of dopamine on OHCs [43]. Others suggested that changes the OAEs abnormalities can be the result of PD pathology and the dopamine deficiency in the lower brainstem [44].
In this study, cognition was assessed using both MMSE and MoCA tests. MMSE is the most commonly used measure for bedside test for screening cognitive function. However, many memory clinics and neurologists use both MMSE and MoCA tests to screen cognition. Both are brief. MoCA test is also more sensitive and pick up more deficits compared to MMSE (e.g. in working memory and executive and visuspatial functions) [32]. Our results showed that ~50% of patients with PD had MCI which is consistent with many studies [2,3,7]. Imaging studies revealed that the early dopaminergic uptake changes within frontal structures (i.e. frontostriatal circuit) are critical to cognitive and executive function and their compromise can be the cause of cognitive impairment in early stages of PD [2,7]. Cognitive deficits in PD are also related to loss of cholinergic neurons in the nucleus basalis of Meynert [8]. Attention deficits are related to both cholinergic dysfunction [8] and dopaminergic pathophysiology. Impairments in semantic verbal fluency, visuospatial ability and working memory are related to the involvement of the temporal lobe and the posterior cortical area by the PD pathology [2,7].
In this study, we assessed central auditory perception using a battery of tests which included SRT, DDT, DPT and SPIN. In this study, testing of speech perception in quite was done by SRT test of speech audiometry [45]. In general, there are number of tests which were constructed to assess different patterns of central auditory processing. Each test has different degree of difficulties and shows good sensitivity and specificity to determine the pattern(s) of the central auditory processing impairment [46]. It has been indicated that the diagnosis of central auditory processing should not rely on a single test but require a battery of objectives measures which targets different patterns of central auditory processing including auditory identification, auditory discrimination, temporal processing and binaural processing. The DDT, DPT and SPIN tests were chosen to assess central auditory processing because (a) they are commonly in clinical applications for evaluation of central auditory processing. (b) They are relatively simpler tests than others and have high sensitivity, specificity, and test–retest reliability to detect central auditory system in diseases with documented brain pathology, i.e. being abnormal only in patients with documented brain pathology and normal in healthy controls [47]. (c) They have been found to be resistant to mild-to-moderate high-frequency SNHL [48,49] and mild cognitive deficits [50]. (d) The standardized Arabic reliable and validated versions of the three tests are available. (e) Tasks for these tests involve different patterns of central auditory processing including auditory discrimination, auditory identification, auditory spatial perception, binaural integration and divided attention; temporal ordering or sequencing, selective auditory attention, the degradation of temporal aspects (as decoding of speech signals) and auditory memory.
In this study, patients had significantly higher SRT compared to healthy controls. Higher SRT was correlated with increasing age and SDS scores. Previous studies reported that patients with PD frequently had impaired SRT and poor word identification compared to healthy controls [11,19]. Troche et al. [19] reported that patients with mild to moderate stages of PD had decreased ability to notice small changes in the amplitudes of pure tones. This was marked for perceptually small intensity differences (e.g. 6 dB), but not for large intensity differences (e.g. 12 dB). Vitale et al. [11] evaluated 45 patients with PD and 45 age-matched healthy controls using SRT and Word Recognition Scores (WRS) tests. The authors reported that the followings: (a) Patients with PD had similar levels of high frequency SNHL as the healthy controls. (b) ~50% of patients required higher levels of stimulus intensity to correctly repeat half of the presented words (RT ear in PD=37.0±12.9, versus 29.9±13.22 for controls; Left ear for PD=39.2±14.14 versus 29.3±16.9 for controls). (c) Patients also had more errors in WRS compared to controls (49% for PD versus 78% for controls). (d) Impairments in SRT and WRS were correlated with higher H & Y scores. In contrast, some studies did not find differences between PD and healthy controls in measurements of speech in quiet [17,51-53].
In this study, the dichotic listening task series of double-digit pairs (two digits at a time) presented to both ears simultaneously using headphones (i.e. free recall DDT). The conventional modes of DDT are (a) the free recall test: this dichotic listening requires the ability to use spatial cues in one auditory localization task. This requires binaural integration and is also referred to as the free recall or divided attention (free recall condition). Binaural interaction almost occurs simultaneously at the levels of the superior olivary complex, the nuclei of the lateral lemniscus and the inferior colliculus; and (b) the directed left and directed right DDT, in which the subject reports only the two digits presented to the directed ear. This dichotic listening task requires binaural separation and is also referred as directed attention or selective allocation attention (right/left ear recall condition) [54]. In this process, the auditory input from either ear crosses over to the contralateral cerebral hemisphere, with ipsilateral inputs being automatically inhibited. Neuroimaging analysis during application of dichotic listening tasks for testing directed attention revealed associated activity in the primary auditory cortices, posterior superior temporal gyri, inferior parietal lobules and inferior and medial frontal gyri. They observed that activation of the superior temporal gyrus, planum temporale, and the inferior parietal lobules were predominantly involved in stimulus selection; and the medial frontal regions were involved in initiation of behavioral responses, and inferior frontal guri were involved in sustained behavioral activity [55].
In general, dichotic listening tasks are among the most widely used behavioral tests for evaluation of central auditory processing. They have been incorporated in almost all of the models and test batteries for auditory central processing. The most commonly used dichotic paradigms are Staggered Spondaic Word (SSW) test, Dichotic Sentences, Dichotic Sentence Identification and Dichotic Words [56].
In this study, we applied the free recall mode of DDT. The reported scores in age-matched healthy controls were ranged from 85% to 100% (versus 60% to 80% for PD). Patients with PD reported poor discrimination of digits and higher number of incorrect responses compared to their age-matched controls (P = 0.0001). Previous studies which applied digit listening tasks reported that patients with PD had significantly lower number of correct responses, increased number of incorrect responses, impaired discrimination of target words and abnormalities in laterality index (right/left ear recall condition) compared to agematched healthy controls [16,25,26]. Richardson et al. [25] reported that the majority of patients with PD (68.75% or 11/16) had lower number of correct responses and/or the laterality index in dichotic presented word pairs compared to healthy controls. Sharpe [26,27] evaluated dichotic listening in 14 patients with PD. They were in H&Y stage I to II and had a mean duration of PD of 4.2 years. The dichotic task consisted of word pairs either contained the target word or a phonemic distractor paired with a phonetically unrelated word. The patients were studied in either a divided attention mode [26] or a selective attention mode [27]. In the divided attention mode, patients with PD discriminated significantly less target words compared to healthy control [27]. In the selective attention paradigm, patients discriminated similar percentage of target words as healthy controls in the attended ear. The authors observed that patients performed more false positive errors to phonemic distractor stimuli presented in the unattended ear only compared to controls but the difference did not reach a significant level between the two groups [26]. The authors reported a comparable right ear advantage in patients with PD which was a similar finding in healthy controls [26,57]. In general, normal-hearing subjects demonstrate a Right-Ear Advantage (REA) [54]. Lewald et al. [16] investigated patients with PD using a dichotic pure-tone pulses as sound stimuli. They did 20 practice trials prior to data collection. The authors did differences in inter-aural time (following a quasi-periodic order) for the sound stimuli between trials. Sound images evoked by these stimuli appeared inside the head, along the line joining the right and left ears. The authors instructed a subject to response to the sound stimuli by pressing a right or left key with respect to median plane of the head. The authors observed significant reduction of the acuity of sound lateralization in PD compared to controls. They also observed that the difference in the recorded inter-aural time was ~2 times longer for PD than healthy controls. It has been suggested that the poor performance in DDT in patients with PD may reflect the overall reduction in the speed of mental processing due to a potential role of the basal ganglia in spatial hearing functions. In contrast, some studies did not find differences between PD in different stages of the disease and healthy controls in measurements for a task using 1-3 dichotic listening tests that probe auditory divided attention [13,24,57].
In this study, the listening task in DPT was to discriminate sounds and characterize the sequences of three tones, one of which differs from the other two in the sequences by being either longer or shorter. DPT is used to test sound discrimination and temporal ordering or sequencing which refers to the processing of multiple auditory stimuli in their order of occurrence. The pattern perception is the result of interaction between the right hemisphere, the transfer through the corpus callosum and the sequencing and verbal labeling in the left hemisphere. The correct pattern perception requires intact right and left hemispheres and intact inter-hemispheric connection which is important to codify duration patterns. If one of the hemispheres is not working appropriately, the conduction of information through the corpus callosum to the other hemisphere is impaired [38,58,59]. Attention and memory are also required for the correct response in DPT. Auditory memory is a process that allows acoustic information to be obtained, stored and archived. It is the function of the anterior temporal region, including hippocampus, amygdala and frontal lobe [60]. In this study, we observed that the scores in DPT were lower in both patients as well as healthy controls compared to their scores in DDT and SPIN tests. This reflects the greater complexity of DPT than DDT and SPIN test. The reported scores in age-matched healthy subjects were ranged from 68% to 80% (versus 30 to 50% for PD). Patients performed worse than age-matched controls in DPT (P=0.001). They had difficulty to identify the order of the three tones and increased number of incorrect responses [23,24]. Lopes et al. [24] evaluated 34 patients with PD at H&Y stage I to II using DPT. The authors reported that younger patients (age 42-64 years old) had more difficulty to identify the order of a sequence of three pure tones (e.g. LSS) compared to healthy controls. The authors did not observe this finding in older patients with PD.
In this study, the SPIN task was series of sentences that are pre-recorded with a noisy background and the subject was instructed to repeat them verbally. Some authors used word (WIN) instead of sentences (SPIN) to test speech perception in noise. In WIN, the subject is asked to repeat a list of words presented in noise. Both WIN and SPIN tests are used to assess selective auditory attention which means to selects relevant auditory information and suppresses irrelevant signals for the task at hand [61]. Repeating sentences instead of words involve multiple auditory perceptual issues other than selective attention including recognition versus recall, temporal processing (as decoding of speech signals and ordering) and memory [50]. Decoding of speech signals refers to phonemic detection and recognition. It is a function of posterior area of the left temporal lobe area. The results of WIN and SPIN tests are examples of interaction between the prefrontal cortices (BA9, BA10 and BA46) and auditory association cortices (BA22). In clinical practice, SPIN test is commonly used as a prognostic factor in rehabilitation of hearing aids and cochlear implant recipients, particularly those without severe memory deficits. In this study, the score of SPIN in healthy controls was 90% to 100% (versus 40% to 90% for PD). Patients with PD performed worse than age-matched controls in SPIN test (P=0.001). They showed inability to understand and repeat sentences. Few studies evaluated speech intelligibility in noisy environment for patients with PD and found that patients encountered troubles to perceive and differentiate between auditory cues and to understand speech particularly in presence of competing stimuli [20,22]. Some studies also reported that in noisy conditions, patients with PD expressed increased vocal loudness in speech intelligibility testing [21]. In contrast, some studies reported no significant differences between patients with PD and healthy controls in WIN test [11,13].
The majority of the above-mentioned studies evaluated patients with PD in early stages of the disease and the patents were on their dopaminergic medication during examination. Most of the above-mentioned studies did not consider the effect of disease progression or the effect of dopaminergic medication on speech processing in degraded listening conditions. We suggest that the contradictory results might be due to difference in selected patients (e.g. early versus advanced disease stages) and varying methodologies and tasks of measurements for auditory processing (e.g. tones, consonant-vowels, digits, words or sentences, etc).
The results of this study indicated that patients in early stages of PD had central auditory perceptual impairments regardless of age, peripheral hearing impairment or cognitive deficits. The deficits in dichotic listening and temporal ordering could both be related to abnormalities of bilateral auditory cortex and inter-hemispheric function, as well as abnormalities in the brainstem by PD pathology and related neurotransmitters’ disturbances. It has been indicated that DPT is more likely to be due to abnormal in brainstem lesions [48]. The deficits in speech intelligibility in noise could be related to the dysfunction of the prefrontal areas and auditory association cortices by the disease process [58].
The results of this showed that only lower scores in cognition were significantly associated with lower scores of central auditory processing. Previous studies indicated that central auditory processing is linked to cognition. This is supported by the followings: (a) there is an interaction between attention, hearing perception and higher-level cognitive processing (i.e. auditory cognitive perception) [49,60,62]. The interaction of prefrontal cortices with auditory association cortices (BA22) is an excellent demonstration of prefrontal executive function and the global cognitive tasks [63]. (b) Neuropsychological and imaging studies have indicated that the frontal cortical regions of the brain and their links with the basal ganglia are critical to executive function and attention [60]. (c) It has been indicated that there is neurochemical reciprocity between dopamine in the prefrontal cortex and striatum. Different cognitive functions are linked to distinct optimum levels of dopamine [64,65]. (d) Studies indicated that auditory processing predicts cognitive decline and auditory deficits have been proposed as early risk markers of dementia [66,67]. (e) It seems that there is bidirectional correlation between cognitive deterioration and auditory perceptual disorders [60,67]. Previous studies (cross sectional and prospective) reported significant correlation between poor performance on dichotic listening tests and cognitive decline in patients with PD reported [16]. Dichotic listening requires attention, short-term memory and executive function and impairment of any of these cognitive domains results in defective speech recognition ability [68]. On the other hand, it has been suggested that adults who perform poorly on dichotic measures should be screened for cognitive impairment [67]. Furthermore, the discrimination of subtle differences in the duration and frequency of syllables, tasks DPT [11] and speech intelligibility and comprehension are influenced by sustained auditory attention, executive functions and auditory associative function which may be impaired in PD [60]. (f) It has been indicated that patients with untreated hearing loss can rely on auditory perceptual processing to determine some cognitive processes as working memory. On the other hand, progressive cognitive deterioration may occur in patients with auditory processing disorder which can be due to exhaustion of cognitive reserves [62]. We suggest that early screening of patients with PD for central auditory perceptual function will help in early patients’ management (i.e. auditory rehabilitation and pharmacotherapies and supplements) not only to improve communication and social behavior but also to improve cognition and slow the progressive cognitive deterioration which commonly occur in many patients with PD. Rehabilitation can include improved comprehension of conversations through media programs and services, amplification via hearing aids, cochlear implants, or other devices. Supplements include vitamin B, lipoic acid, coenzyme Q10, ginco biloba and others.
Limitations of the study
This study had limitations which include: (1) the small sample size: this could be explained by the long list of inclusion and exclusion criteria. Many patients were excluded as being elderly, in advanced stages of the disease, had comorbid medical conditions, on multiple drug therapies for treatment of PD among were drugs which greatly compromise cognition [32]. Also many patients could not tolerate multiple auditory testing and did not complete the battery test. (2) The lack of a comparative drug-naïve or patients who were “off phase medications” to distinguish the patterns of cognitive deficits due to the disease itself versus the response or the effect of dopaminergic medications. In clinical practice, it seems difficult to recruit a good number of drug-naïve patients. Also examining the patient during the off medication is difficult for ethical concerns (e.g. increased symptoms, manifestations of weaning off, motor fluctuations, etc).
Results of this study indicated that central auditory perceptual dysfunction can occur in early stages of PD and independent to peripheral hearing loss or cognitive impairment. In some patients, they may occur before MCI. The DDT, DPT and SPIN are useful battery measures for testing central auditory functions in patients with PD. We recommend screening for central auditory perceptual function in early stages of PD. They may help in patients’ management (i.e. pharmacotherapy for hearing impairment, or auditory rehabilitation) and may slow or prevent progressive cognitive decline. Dopamine deficiencies in PD at different auditory pathway levels including the brainstem and cortico-subcortical level and neurodegenerative diffuse PD pathology are the causes of central auditory processing impairments.
Abbreviations: BDI-II: Beck Depression Inventory II; DDT: Dichotic Digit Test; DPT: Duration Pattern Test; Hoehn and Yahr Scale: H & Y Scale; IHCs: Inner Hair Cells; LOC: Lateral Olivocochlear; MMSE: Mini Mental State Examination; MOC: Medial Olivocochlear; MoCA: Montreal Cognitive Assessment; NMMs: Non-Motor Manifestations; OAEs: Otoacoustic Emissions; OHCs: Outer Hair Cells; PD: Parkinson’s Disease; PDD: Parkinson’s Disease Dementia; PTA: Pure Tone Audiometry; SDS: Speech Discrimination Scale; SNHL: Sensorineural Hearing Loss; SPIN: Speech in Noise; SRT: Speech Reception Threshold; WIN: Word in Noise.
Declaration of funding: This work was not funded.
Financial/other relationships: The authors declare no conflict of interest. The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Author contributions: S.A.H, M.A.A, A.M.O and M.K.S.M. designed the conception, had full access to raw data, and verified the underlying data and interpretation of the results and final approval of the manuscript. S. A. H and M. K. S. M did the neuropsychiatric interviewing and applied the measurements for depression and cognition on participants. A.M.O did the ENT and audiological evaluations, and applied the basic audiologic and central auditory processing testing on participants. S.A.H wrote the manuscript and had the final responsibility to submit it for publication.
Data availability statement: Datasets of this work will be available from the corresponding author (SAH) upon reasonable request.
Consent for publication: All participants approved to publish this work.
